what teaching does the nurse provide to a patient who had outpatient surgery for hallux valgus?
- What is hallux valgus?
- Indications for surgery: When does hallux valgus require surgery?
- Hallux valgus surgery is e'er a custom procedure
- The goal of hallux valgus surgery: Pain-free and nicely shaped feet
- Which doctors perform bunion surgery?
- What is the success rate of bunion surgery?
- Preparing for bunion surgery
- Surgical methods for correcting hallux valgus
- What type of anaesthetic is used for surgery of the large toe?
- Should I await pain after the surgery?
- What will my stay be like at Gelenk-Klinik?
- Outlook and complications following hallux valgus surgery
- What exercise I need to go along in mind later surgery?
- Rehabilitation following hallux valgus surgery
- What is the price of bunion surgery?
- Who is bunion surgery suitable for?
- How tin international patients schedule bunion surgery?
- FAQ: Ofttimes asked questions well-nigh hallux valgus surgery
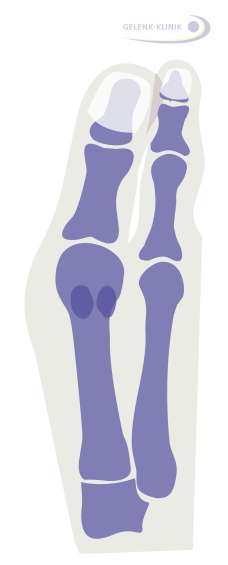
 Fig. 1: Hallux valgus surgery corrects a misalignment of the large toe. Usually the os in the large toe is corrected in conjunction with the correction of the soft tissue of the joint sheathing of the metatarsophalangeal joint. © Gelenk-Klinik.de
Fig. 1: Hallux valgus surgery corrects a misalignment of the large toe. Usually the os in the large toe is corrected in conjunction with the correction of the soft tissue of the joint sheathing of the metatarsophalangeal joint. © Gelenk-Klinik.de
Is your large toe leaning more than and more outwards, crowding the smaller toes on your foot? Practise your feet hurt subsequently longer walks or oftentimes fifty-fifty at the offset of the day? Is this hurting restricting your flexibility and mobility in your daily activities? Then just similar so many of the other - mainly female - patients of our foot and ankle section, you're suffering from hallux valgus (bunions).
The experts in our foot department specialise in the gentle treatment of misalignment of the big toe with minimally invasive procedures on the forefoot. What is particularly of import to our many patients from Germany and abroad is: Information technology significantly speeds healing and rehabilitation and prevents complications.
The goal of hallux valgus handling is this: We desire our patients to regain their mobility as quickly every bit possible and experience permanent medical and cosmetic improvement of their hallux valgus.
The more severe the hallux valgus deformity, the more circuitous the surgery will be. That is a reason to encounter a specialist for gentle options to correct hallux valgus early.
What is hallux valgus?
Hallux valgus (bunions) is a very widespread misalignment of the big toes. The large toe noticeably drifts to the outer border of the foot, where information technology also crowds the smaller toes. With the hallux valgus deformity the metatarsophalangeal joint is overstrained and as a result painful →arthritis of the large toe (hallux rigidus) can develop.
The protruding bunion at the metatarsophalangeal joint becomes inflamed and painful and tin bang-up. There are numerous conservative procedures to treat hallux valgus and to alleviate pain.
Indications for surgery: When does hallux valgus require surgery?
What causes Hallux valgus pain?
- The bunion, tender to pressure, becomes inflamed and pushes against the inside of the shoe.
- The crowded minor toes (hammer toes and claw toes) cause farther forefoot deformities.
- Hurting occurs in the arch of the foot, because the big toe is no longer existence fully utilised and the small-scale toes are overstrained.
- Arthritic hurting in the metatarsophalangeal joint occurs due to wear of the joint.
Hallux valgus is a cosmetic problem for many female patients - specially in open-toed shoes. But cosmetics lone are not a reason to operate on this misalignment. When planning and performing this plastic surgery of the large toe nosotros do, nevertheless, pay great attending to an appealing corrective consequence. This allows us to fully restore the quality of life of our patients.
I requirement for surgery is a painful misalignment. This is a misalignment of the big toe. This can also not be treated by changing shoes, using insoles or foot exercises. Although insoles may provide relief for painful hallux valgus. However, they practise not correct the misalignment.
Corrective goals of hallux valgus surgery
- Straightening the big toe.
- Correcting hammer and claw toes.
- Removing the swollen brawl of the human foot (removal of exostosis).
- Minimal surgical scars in the visible expanse.
Only when the anxiety have a significantly lower weight begetting capacity in everyday life, the bunion are already painful and mobility restricting, it is medically justified to recommend the operation.
Hallux valgus is a cosmetic problem for many female person patients - specially in open-toed shoes. Merely cosmetics alone are non a reason to operate on this misalignment. When planning and performing this plastic surgery of the big toe we do, withal, pay dandy attention to an appealing cosmetic outcome. This allows usa to fully restore the quality of life of our patients.
One requirement for surgery is a painful misalignment. This is a misalignment of the big toe. This tin can likewise not be treated past changing shoes, using insoles or human foot exercises. Although insoles may provide relief for painful hallux valgus. However, they do not correct the misalignment.
Hallux valgus surgery is always a custom procedure
Comorbidities of hallux valgus to exist included in therapy
- Bunion
- Osteoarthritis of the big toe (metatarsophalangeal joint (hallux rigidus).
- Bursitis (bursa inflammation) on the toe pads.
- Bursitis at the adjacent lesser toes.
- Painful overload the lesser toes
- Claw toes
- Hammertoes
Hallux valgus is always a combination of various pathological processes. The misalignment of the big toe is accompanied by, for instance, peel alterations and bursitis. The crooked big toe crowds adjacent small toes. This results in painful strain. We want to gain an agreement of the patient's specific condition through thorough diagnosis before planning surgical treatment. Beneath we would like to present an overview of the standard hallux valgus surgeries. But first nosotros would like to stress each patient'south specific case and lifestyle bear on the decision whether to perform the hallux valgus surgery.
An experienced specialist plans the specific hallux valgus surgery and agrees information technology with the patient.
Hallux valgus animation
Combination of hallux valgus surgeries
Most hallux valgus surgeries consist of several of the post-obit procedures:
- Repositioning the os (osteotomy):
This straightens the pes ray. - Soft tissue correction (lateral release):
A rigid misalignment can exist straightened by correcting the joint sheathing. - Tendon correction:
The length of the tendon must be corrected so the pull of the tendon does non deform the big toes over again. - Treating the metatarsophalangeal articulation:
Articulation-preserving cheilectomy (removing bone spurs) or fusing the metatarsophalangeal joint (arthrodesis) for severe arthritis.
The orthopaedist will merely consider hallux valgus surgery one time all conservative hallux valgus treatments have been exhausted. Long-term effects of hallux valgus often include arthritis of the metatarsophalangeal joint: This sometimes besides ends in limiting the flexibility of the metatarsophalangeal joint.
How can a patient prevent hallux valgus surgery?
Switching to healthy shoes with a large toe box and consistent conservative hallux valgus treatment can delay the progression of hallux valgus. Therefore once you notice a hallux valgus deformity you shouldn't wait too long to offset treatment.
What to do if conservative hallux valgus treatment doesn't provide relief?
Increasing stiffness of the big toe joint and the misalignment of the adjacent toes of the foot make hallux valgus more complex to operate on over time.
Long-term complications such as hallux rigidus (arthritis of the metatarsophalangeal joint) increase in severity.
Post-obit hallux valgus surgery most patients are glad to no longer have to endure the pain, limping and cosmetically unattractive misalignment.
The goal of hallux valgus surgery: Pain-free and nicely shaped feet
 of the big toe flexor tendon can be seen in an off-centre position below the metatarsophalangeal joint: They no longer surround the bone of the toe symmetrically but have instead shifted. The draw of the tendon is therefore also no longer parallel to the direction of the foot ray. © Dr. Thomas Schneider") Fig. ii: Human foot with hallux valgus deformity: The big toe is noticeably turned outward. The sesamoid basic (small bones resting freely on the tendons) of the big toe flexor tendon can exist seen in an off-centre position below the metatarsophalangeal joint: They no longer surround the os of the toe symmetrically only have instead shifted. The draw of the tendon is therefore besides no longer parallel to the direction of the foot ray. © Dr. Thomas Schneider
Fig. ii: Human foot with hallux valgus deformity: The big toe is noticeably turned outward. The sesamoid basic (small bones resting freely on the tendons) of the big toe flexor tendon can exist seen in an off-centre position below the metatarsophalangeal joint: They no longer surround the os of the toe symmetrically only have instead shifted. The draw of the tendon is therefore besides no longer parallel to the direction of the foot ray. © Dr. Thomas Schneider
In addition to straightening the big toe, the goal of treating hallux valgus (bunions) surgically in early stages is to preserve the metatarsophalangeal joint at risk of developing arthritis. So hallux surgery permanently corrects the hallux valgus deformity. The function - the natural gait - can only be restored once the anxiety are returned to their natural shape: In a healthy gait the human foot rolls off beyond the big toes. This rolling motility is distorted in hallux valgus. The small toes assume this rolling movement: This stresses them, deforming them over fourth dimension.
The hallux valgus-induced crooked bone axis of the big toe is straightened through hallux valgus surgery. The pull of tendons and muscles is normalised through hallux valgus surgery. Otherwise with hallux valgus they would pull the big toe more to the side with every pace. Information technology's therefore of import to operate gently on the muscles and tendons surrounding the big toe and injure them as little as possible during hallux surgery.
The distorted alignment of the joint is restored as much as possible. Hallux surgery permanently improves the inward rotation of the toe(pronation).
- Reduce hurting
- Visual correction of the shape of the foot
- Straightening the base of the big toes
- Preventing osteoarthritis (Hallux rigidus)
- Enabling the patient to wear open up shoes again
- Minimally invasive procedure to minimise scarring
During hallux valgus surgery nosotros also ever consider the position of the sesamoid basic: A sesamoid bone (lat. Os sesamoideum) is a small os which rests on the tendon. These sesamoid bones freely suspended by the tendons are small spacers betwixt the tendon and the os. They ensure the minimal distance to the os necessary for optimal tendon function. Hallux valgus surgery as well needs to adjust the position and role of the sesamoid basic: The sesamoid bones impact the misalignment of the big toe due to the depict of the tendon, which in turn intensifies the hallux valgus.
Which doctors perform bunion surgery?
Hither at Gelenk-Klinik we believe a close relationship between surgeons and patients is important. This means you volition be in the care of your attention physician from discussing your medical history until afterward the surgery. Y'all volition therefore have one contact person who is very familiar with your case and who will be assigned to you throughout your stay at Gelenk-Klinik. Our pes and ankle surgery experts are Dr Thomas Schneider and Dr Martin Rinio. They are certified foot and ankle surgeons and their continuing education, diagnosis skills and surgical quality are reviewed annually by an independent High german expert clan. The orthopaedic Gelenk-Klinik therefore bears the championship of "Zentrum für Fuß- und Sprunggelenkschirurgie" (ZFS) [Foot and Ankle Surgery Center].
What is the success rate of bunion surgery?
The success of the surgery is non determined past the severity of the deformity of the big toe. However, the severity of the bunion does affect the surgical procedure: the more severe the deformity, the further back on the metatarsophalangeal bone we volition need to correct the position of the large toe. The more severe the deformity, the more than we use stabilising metal implants. The healing process and afterward-care are then also correspondingly longer. The metal may also need to be surgically removed after vi to 12 months. Still, fifty-fifty with a severe deformity, osteoarthritis of the big toe can be prevented simply equally effectively as with a mild deformity.
The potential benefits and complications of bunion surgery must always be weighed upwardly carefully. In international studies on this consequence, about 80% of patients felt very well post-obit surgery. Another x–fifteen% felt better than before surgery, even if they yet had small-scale problems. Only virtually 5% of all the patients in the studies experienced no improvement from bunion surgery. The more than experienced the surgeon, the greater the likelihood bunion surgery will provide a adept effect.
In our experience, intensive follow-up work with foot exercises, which every patient can easily do at home, can significantly meliorate the event of bunion surgery. Exercise sheets and instructions are available from the Gelenk-Klinik foot clinic.
Preparing for bunion surgery
The dr. will get-go perform detailed medical diagnostics to obtain a good overall picture. In addition to reviewing the medical history and a physical examination, this also includes taking X-rays whilst standing, i.e. while the foot is begetting weight. Measuring the intermetatarsal angle (angle between the 1st and 2nd metatarsal bone) allows the physician to decide the severity of the big toe deformity. This measurement will then exist used to determine a suitable surgical procedure together with the patient.
Later determining the patient is fit for surgery, the treating medico will explicate the procedure and possible complications of surgery. The patient volition also come across with the anaesthetist, who will make a detailed assessment every bit to whether the patient is healthy enough for anaesthesia. One time approved by the anaesthetist and the surgeon, the surgery can typically be performed the day afterward the examination.
Surgical methods for correcting hallux valgus
In that location are several internationally established and proven surgical methods for correcting hallux valgus, which nosotros besides employ at the orthopaedic Gelenk-Klinik.
The more severe the misalignment, the more than complex the surgery will exist
The post-obit principle applies: The more astringent the misalignment, the farther back on the foot ray the big toes need to be operated on and corrected. The more severe the misalignment, the longer the healing procedure and follow-up treatment will be. With a severe misalignment, which is often accompanied by arthritis of the big toe, the long-term result and the load-bearing chapters are also the same as after minor misalignment.
The surgical options for minor misalignment showtime in front of the metatarsophalangeal joint. For a moderate misalignment the surgery is performed on the metatarsal bone. For astringent hallux misalignment the repositioning or fusion is performed at the metatarsophalangeal joint: This is the connection between the metatarsal bone of the foot ray and the tarsal bone.
These hallux valgus surgery techniques aimed at the positioning of the big toe and the metatarsophalangeal joint are always accompanied by associated procedures on the soft tissues (muscles, capsules and tendons).
Which technique is used for each individual case depends on the anatomic location of the deformity and the severity of the misalignment. The orthopaedist chooses the suitable hallux valgus surgical method together with the patient: The options for treatment are discussed with the patient based on the thorough medical examination and the ten-ray diagnosis.
The various techniques are used depending on the severity of the hallux valgus misalignment (intermetatarsal angle = angle between the first and 2d metatarsal bone). These hallux valgus surgical methods apply to the anatomic areas shown below.
Surgery behind the metatarsophalangeal articulation
Distal bone repositioning is the preferred corrective measure for hallux valgus.
Minimally invasive hallux valgus surgery for balmy to moderate misalignment
Every bit specialists we always strive to operate with every bit little repositioning of the bone and scarring as possible. Our goal is to correct hallux valgus as soon as possible using only soft tissue procedures. To date this is non notwithstanding entirely possible: Adapted screws and implants for fixing the bones are ordinarily still used.
Minimally invasive surgery is "distal repositioning": so the big toe is repositioned starting at the metatarsophalangeal joint ("distal"). Nosotros particularly like to apply this surgery for mild to moderate misalignments of the big toe.
By using compatible titanium screws, this hallux surgery tin can ordinarily forego follow-upwards surgery to remove the screws. The screws can remain in place without causing problems.
By using compatible titanium screws, this hallux surgery can usually forego follow-upward surgery to remove the screws. The screws can remain in place without causing problems.
This cosmetically very favourable procedure with minimal scarring is used for mild to moderate hallux valgus deformities.
If arthritis of the metatarsophalangeal joint (hallux rigidus) is already present due to the hallux valgus deformity, however, this minimally invasive procedure can no longer be used. In this case, the procedure must include treating the metatarsophalangeal joint.
What is the process used in minimally invasive hallux valgus surgery?
Only two small skin incisions are fabricated at both sides of the large toe. The minor incisions hardly involve the soft tissue. This reduces the healing time and charge per unit of post-operative complications - compared to open up hallux valgus surgical methods - fifty-fifty more.
The minimally invasive hallux valgus surgery realigns the kleptomaniacal foot ray using small instruments, similar to dental instruments. In some other step a small incision opens and widens the joint capsule, which is often shortened due to hallux valgus. This allows the joint capsule to provide the space required by the normal alignment of the big toe.
This "minimally invasive" method has several advantages compared to the other - also minimally invasive - hallux surgery methods. Injury to the soft tissue is significantly less than with other osteotomies. This greatly reduces the healing time and the time until the patient reaches total mobility. Older patients specially do good from this: They return to mobility sooner. Less injury to the soft tissue as well significantly reduces post-operative swelling of the foot compared to other procedures.
Alike osteotomy for mild hallux valgus higher up the metatarsophalangeal articulation
Akin Osteotomie: Step by step
Mild hallux valgus interphalangeus: This is an isolated misalignment of the large toe beyond the metatarsophalangeal articulation © Dr. med. Thomas Schneider
If the phalanx of the pes is misaligned in front of the metatarsophalangeal articulation (hallux valgus interphalangeus), a and then-called Akin osteotomy may as well be performed.
During Akin osteotomy the big bone of the big toe is repositioned beyond the metatarsophalangeal joint (metatarsus interphalangeus). The change in direction through repositioning surgery. Alike osteotomy oftentimes does not address the actual cause for the hallux valgus deformity: The misalignment of the metatarsal bone. Since it only corrects the large toe, we therefore typically apply Akin osteotomy in conjunction with other hallux valgus procedures.
With Akin osteotomy the repositioning is always accomplished past removing a wedge from the phalanx of the human foot. The phalanx of the pes then grows dorsum together in a new, desired position.
Correcting the alignment following Akin osteotomy besides allows the pull of the tendons in the big toe to exist normalised once again.
Corrections of the metatarsal bone (metatarsal correction)
Chevron osteotomy: Hallux valgus surgery of the metatarsal bone for mild hallux valgus deformities
![]() Fig. 7: Planning for repositioning the bone (osteotomy) in Chevron surgery across the metatarsophalangeal articulation. With Chevron osteotomy a V-shaped cut is made behind the showtime metatarsal head. It is so moved outward and secured in place with a small titanium spiral. © Dr. Thomas Schneider
Fig. 7: Planning for repositioning the bone (osteotomy) in Chevron surgery across the metatarsophalangeal articulation. With Chevron osteotomy a V-shaped cut is made behind the showtime metatarsal head. It is so moved outward and secured in place with a small titanium spiral. © Dr. Thomas Schneider ![]() Hallux Valgus, korrigiert durch Chevron-Osteotomie mit Fixierung durch selbstschneidende Titanschraube © FH-Orthopaedics
Hallux Valgus, korrigiert durch Chevron-Osteotomie mit Fixierung durch selbstschneidende Titanschraube © FH-Orthopaedics
The Chevron osteotomy is suitable for moderate hallux misalignments. Applying the Chevron method requires arthritis in the metatarsophalangeal joint to exist no more than than moderate. With the Chevron method a V-shaped wedge is removed at the level of the metatarsal head. The metatarsal head is moved outward and secured in place with a screw (titanium). The joint sheathing is gathered at the inside to facilitate the regular orientation of the big toe.
In mild hallux valgus deformity (< 17°) at that place are no pregnant changes to the joint still (e.g. arthritis in the big toe joint). In this case Chevron osteotomy is very suitable. Then Chevron osteotomy is used for mild to moderate types of hallux valgus.
Performing the Chevron osteotomy
With Chevron osteotomy, first a small skin incision is placed across the metatarsophalangeal joint at the back of the foot. And then the tendons and the joint capsule, shortened due to the hallux misalignment, are discrete and widened (soft tissue procedure). The shrinking of the tendons and articulation sheathing intensifies the misalignment of the big toe in hallux valgus.
And then the protruding ganglion is ablated using a minor saw or a chisel.
An incision is placed at the offset metatarsal bone at the level of the metatarsal head. The metatarsal head is moved to the correct position, outward toward the small toe, until it lies below the sesamoid bones.
The next step in the Chevron osteotomy is to secure the phalanx of the foot in identify with a self-tapping titanium spiral or wire.
And then the joint capsule is tightened. The small titanium screws usually remain in the phalanx of the pes: They typically do not need to be removed. Follow-upwards surgery for hallux valgus surgery to remove the screws is commonly avoided, if possible. However, if the titanium screws do crusade issues, they tin be removed later on no less than iii months through minor outpatient surgery.
 Fig. 9: Lateral view of Chevron osteotomy: The osteotomy is fixed by self-tapping titanium screws. The foot ray can and then heal in the new alignment. © Dr. Thomas Schneider, Medico
Fig. 9: Lateral view of Chevron osteotomy: The osteotomy is fixed by self-tapping titanium screws. The foot ray can and then heal in the new alignment. © Dr. Thomas Schneider, Medico
More severe misalignments oftentimes too involve changes to the articulation at the joint capsule. Soft tissue surgery is therefore typically performed along with the repositioning of the bone.
In Chevron osteotomy the lateral shift in the large toe is express. To prevent relapses, it's advisable to review the effect of the hallux valgus correction during surgery using an paradigm converter. This allows the specialist to review the verbal position of the sesamoid os.
Scarf osteotomy: Surgery for moderate to severe hallux valgus
Scarf osteotomy is for moderate to astringent hallux valgus deformities. The metatarsal bone of the first foot ray is visible on the inside of the foot following a skin incision. During the osteotomy it is cutting in a Z-pattern (repositioning of the os). It is then secured in a new direction using small screws. Hither, a soft tissue procedure (gathering) of the joint sheathing of the metatarsophalangeal joint may too exist required.
Bunion correction with Scarf and Akin osteotomy
The so-called Scarf osteotomy is very well suited for correcting moderate to severe types of hallux valgus (from 17° to over 40°).
Scarf osteotomy tin can likewise correct the rotation in the longitudinal axis of the big toe which often occurs in hallux valgus.
Scarf osteotomy besides combines the correction of the variance in the bone in hallux valgus with surgery of the soft tissues (tendons and sheathing).
Performing the Scarf-Osteotomie:
In scarf osteotomy the peel incision is placed at the inside of the human foot, from the base of the toe to the base of the metatarsal os. So a Z-shaped wedge is sawn out at the side, at the diaphysis of the first metatarsal os. During Scarf osteotomy the role of the big toe with the joint - the so-called metatarsal caput - is moved outward along the cut edge. This allows information technology to be moved to the correct bending.
To let this shift without tension, the tendons pulling the big toe toward the middle, is moved.
The outside of the joint capsule which is also deformed in hallux valgus is released.
The bone is then secured with two small titanium screws.
The extensive bone contact allows the bone to heal well. The titanium screws typically remain in place and do not crave removal. Nevertheless, if they do crusade problems, the screws can be removed later no less than three months through minor outpatient surgery.
Surgery of the metatarsophalangeal joint
Advanced arthritis of the metatarsophalangeal articulation (MTPJ) requires surgery.
With joint-preserving cheilectomy the metatarsophalangeal joint can be cleaned arthroscopically and bone spurs removed.
With an arthrodesis of the metatarsophalangeal joint is fused.
A metatarsophalangeal joint can also be treated with a hemi-prosthesis of the metatarsophalangeal joint.
Lapidus arthrodesis: Surgery of the tarsometatarsal joint
The Lapidus arthrodesis is considered in very severe cases of hallux valgus deformity with concurrent arthritis or instability in the metatarsophalangeal joint of the beginning metatarsus with the tarsal os.
Lapidus arthrodesis is particularly helpful for major misalignments of the large toe with a peculiarly big intermetatarsal bending (>40°). Lapidus arthrodesis tin also be used for arthritis of the tarsometatarsal joints.
What type of anaesthetic is used for surgery of the big toe?
We typically perform bunion surgery under general anaesthesia. Even so, nosotros can as well perform information technology nether spinal anaesthesia if the patient would adopt to avoid general anaesthesia. In this case the anaesthetist injects the anaesthetic into the vertebral culvert of the lumbar spine. Here, the patient is conscious during surgery. You lot will be able to decide the best anaesthesia for you together with the anaesthetist. Our anaesthetists are very experienced in both methods and cull the option all-time suited for the patient and their requirements during a pre-operation discussion.
Should I expect pain afterwards the surgery?
Any procedure causes pain. We always strive to minimise pain later on bunion surgery. The corresponding anaesthetist volition often use a so-called nerve block earlier the surgery, numbing the respective foot for around thirty hours. This step alone manages the majority of the pain, and any residue discomfort can then be easily treated with typical medication. Our goal is for you to feel as trivial pain as possible.
What will my stay exist like at Gelenk-Klinik?
 Private room in the Gelenk-Klinik in Gundelfingen, Frg
Private room in the Gelenk-Klinik in Gundelfingen, Frg
During your inpatient stay at Gelenk-Klinik you will have a single-occupancy room. The room has a bathroom with a shower and a toilet. All rooms include towels, a bath robe and slippers. They likewise feature a mini-bar and a safe. All of the rooms are moreover fitted with a television. You only need to bring your personal medication, comfortable clothes and sleepwear. Later on surgery you will receive 24-hour care from experienced nursing staff and experienced physiotherapists. The inpatient stay post-obit bunion surgery is typically 2 days. There is a hotel within walking distance where your family unit members tin stay. We are happy to brand reservations for you.
Outlook and complications following hallux valgus surgery
Potential postoperative complications
- Chronic pain even after surgery.
- Painful irritation due to screws or wires.
- Lesions due to redistribution of the load when walking.
- Stress fractures due to the load change post-obit surgery.
- Infection following surgery.
The possible benefits and complications of hallux valgus surgery must always be carefully deliberated. In international studies on this topic about 80% of patients felt very well following surgery. Nearly 10%-15% felt better than before surgery, even if they still had problems. Almost 5% of all patients in the studies experienced no comeback. The more than experienced the surgeon, the greater the likelihood hallux valgus surgery volition provide a good result.
In our feel, intensive follow-up work to hallux valgus surgery with foot exercises significantly improved the consequence.
What do I need to keep in heed after surgery?
You should elevate and ice your pes immediately post-obit surgery to minimise pain and swelling. A special blazon of bandage supports the big toe during the first few days. The stitches volition be removed subsequently about 12 days. In one case these are removed, y'all can also shower once again.
You will also receive a special shoe which takes force per unit area off the forefoot and should be worn for 4 weeks. The heel will bear the full weight of your body. When walking longer distances you lot should also employ crutches to protect your pes. Thrombosis prophylaxes are imperative during the time you lot are unable to put your total weight on the pes. Y'all will as well receive physiotherapy and lymph drainage to prevent muscle loss and minimise swelling of the forefoot. Swelling of the forefoot volition final longer the older the patient.
- Inpatient treatment: ii days
- Optimal length of stay on the premises: 5 days
- Earliest return flight: 5 days subsequently surgery
- Recommended render flight: vii days later on surgery
- Showering permitted: 12 days afterward surgery
- Recommended time off piece of work: iv weeks (depending on job)
- Recommended removal of stitches: 12 days
- Time earlier able to drive again: 4 weeks
Rehabilitation following hallux valgus surgery
 Fig. x: Following hallux valgus surgery, patients are immediately mobile again using a special forefoot offloading shoe. This shoe shifts the entire bodyweight to the heel. This also ways patients are immediately able to travel once again. But patients should besides elevate their foot as much every bit possible whilst the wound is healing to prevent swelling.
Fig. x: Following hallux valgus surgery, patients are immediately mobile again using a special forefoot offloading shoe. This shoe shifts the entire bodyweight to the heel. This also ways patients are immediately able to travel once again. But patients should besides elevate their foot as much every bit possible whilst the wound is healing to prevent swelling.
The healing process typically takes three to six weeks. The more severe the misalignment, the longer rehabilitation will take. An 10-ray examination provides accurate data on the condition of the operated articulation during the follow-up appointment, nearly four weeks after surgery.
All of the corrective surgeries for hallux valgus we perform allow for functional follow-upwards treatment with full weight begetting, using a so-called forefoot decompression shoe, which in turn significantly lowers the take a chance of thrombosis.
one thousand hallux valgus surgery. The special forefoot decompression shoes must be worn for a period of iv to six weeks.
Post-operative rehabilitation
- Redressing bandages
- Night splint
- Thrombosis prophylaxis
- Detumescing measures, peak
- Lymphatic drainage
Notwithstanding the pes should also be elevated and rested as much as possible following hallux valgus surgery: This promotes faster healing.
Eventually a redression splint can be used at night.
After approx. five more than weeks wide shoes may be worn once again. Mail service-operative foot exercises are vital for muscular rest and to stabilise and strengthen the foot.
Self-massaging the arch with a soft lawn tennis ball is highly recommended. Incapacity for piece of work depends on the healing process and the profession.
What is the cost of bunion surgery?
In addition to the cost of surgery you also need to plan for farther costs for diagnosis, medico's appointments and temporary supports (e.g. crutches). These amount between € 1200 and € 1700. If you programme to have the recommended outpatient physiotherapy in Germany after surgery, nosotros will gladly schedule appointments with speciality physiotherapists and obtain an estimate of costs.
Yous volition notice information about the cost of hotel accommodation and any follow-up treatment of the rehabilitation on the websites of the respective providers.
Determination: Who is bunion surgery suitable for?
We crave recent MRI scans and Ten-rays to exist able to fully assess the deformity of your large toe. We volition employ these scans to determine if you are eligible for the procedure. Good apportionment is important for healing after forefoot surgery. The human foot is the furthest motility organ from the heart. The soft tissue drapery of the heavily strained foot is very thin and mechanical strain on the foot very high. Any illnesses which further reduce the naturally low circulation are therefore unfavourable to healing afterward surgery. The following illnesses will prevent or complicate successful bunion surgery:
- PVD (peripheral vascular disease)
- Diabetic foot
- Early onset polyneuropathy (nerve disease often caused past diabetes)
- Venous insufficiency
In these cases nosotros need to take a vein specialist (phlebologist) thoroughly examine the circulation of the human foot before deciding whether or non to perform bunion surgery.
Polyarthritis and rheumatic diseases will non prohibit pes surgery. Even so, they must be considered accordingly when selecting the surgical method. Prior bunion surgery volition also complicate the repositioning surgery considerably and must be taken into account by the foot specialist when selecting the surgical strategy.
 or the diabetic foot syndrome prevent or complicate wound healing after hallux valgus surgery. © Viewmedica") Circulatory disorders are ever a contraindication: Peripheral vascular disease (PVD) or the diabetic foot syndrome forbid or complicate wound healing after hallux valgus surgery. © Viewmedica
Circulatory disorders are ever a contraindication: Peripheral vascular disease (PVD) or the diabetic foot syndrome forbid or complicate wound healing after hallux valgus surgery. © Viewmedica
How tin international patients schedule bunion surgery?
The foot specialists in Germany volition firstly need recent MRI images and in item X-rays of the respective pes to determine the condition of the base of the big toe. Later on sending these to us via our website, y'all will receive patient information including proposed treatment and a bounden cost approximate within ane–2 business days.
Gelenk-Klinik offers appointments for international patients to correspond with your travel itinerary. We will gladly help you apply for a visa once we have received the down-payment specified in the price gauge. If the visa is denied, we will refund the full down-payment. Nosotros endeavor to minimise the time between the preliminary examination and the surgery for our international patients to avoid boosted travel. During your inpatient and outpatient stay our multi-lingual (English, Russian, Spanish, Portuguese) case management team will be there to assist you lot. We can too provide an interpreter (e.g. Arabic) at any time, at the patient's expense. We volition gladly help you lot with organising transportation and lodging and provide recreational tips for your family members.
FAQ: Oft asked questions almost hallux valgus surgery
How long does hallux valgus surgery accept to heal?
Healing is consummate afterward iv to six weeks. Incapacity for work, however, also depends on your job: A standing chore requires more time off than a sitting job.
Can I walk subsequently hallux valgus surgery?
Using a forefoot decompression shoe you lot can walk immediately following surgery. This forefoot decompression shoe prevents the foot from rolling off across the large toe.
Is the foot immobilised following surgery?
The foot is not put in a bandage or immobilised following hallux surgery. The big toe also remains passively flexible.
When can I return to wearing regular shoes?
Even afterwards completing follow-upward handling with the forefoot decompression shoe you should wear soft, comfortable and wide shoes for another 4 to six weeks.
Hallux valgus on both sides: Is simultaneous surgery on both feet advisable?
We only want to offer simultaneous surgery of hallux valgus in emergencies. Unremarkably, having one healthy foot is very important to the rehabilitation of the operated human foot. If surgery is required on both sides, a period of three months between the procedures is sensible and should not be less than that.
Source: https://www.joint-surgeon.com/orthopedic-services/foot-and-ankle/hallux-valgus-hallux-rigidus-bunion-surgery.html
0 Response to "what teaching does the nurse provide to a patient who had outpatient surgery for hallux valgus?"
Enregistrer un commentaire